lung expansion lv rv lressure|Cardiopulmonary physiology: why the heart and lungs are : 2024-10-08 Increased RV pressure and volume leads to interventricular septum flattening or convex bowing into the LV cavity, thus decreasing the LV volume and filling. Clinically important . 26 nov. 2023 — De Audemars Piguet Royal Oak UAE-editie heeft een roestvrijstalen kast met de kenmerkende achthoekige vorm die zo typerend is voor de Royal Oak-modellen. .Chronograph, Date, Minute repeater. Find low prices for 51 Audemars Piguet ref. 26470ST.OO.A101CR.01 watches on Chrono24. Compare deals and buy a ref. .
0 · Using heart
1 · Understanding Heart
2 · The right ventricle under pressure: Anatomy and imaging in
3 · Right versus left ventricular remodeling in heart failure due to
4 · Physiology of Heart
5 · Physiologic Approach to Mechanical Ventilation in Right
6 · Interaction between respiration and right versus left ventricular
7 · Hemodynamic function of the right ventricular
8 · Heart
9 · Cardiopulmonary physiology: why the heart and lungs are
Audemars Piguet launches its first 34 mm Selfwinding Royal Oak. The stainless steel case of this model is enhanced by an elegant silver-toned “Grande Tapisserie” dial.
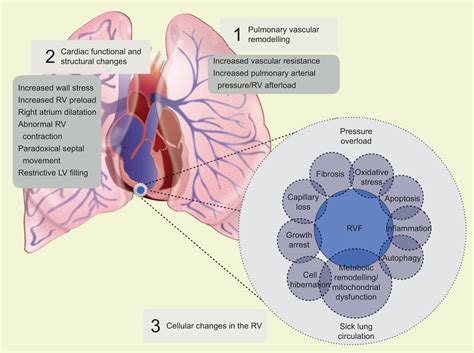
lung expansion lv rv lressure*******Similarly, left ventricular (LV) ejection pressure is estimates as arterial pressure minus ITP. Clearly, both transmural Pra and transmural LV pressure vary with changes in ITP while neither the upstream venous driving pressure, referred to as mean systemic fillingDuring mechanical ventilation, the application of positive pressure produces an increase in zones 2 and 1 at the expense of zones 3 and 2, resulting in the alveolar pressure (P .Increased RV pressure and volume leads to interventricular septum flattening or convex bowing into the LV cavity, thus decreasing the LV volume and filling. Clinically important .
Mechanical ventilation induces cyclic changes in left ventricular (LV) stroke volume, which are mainly related to the expiratory decrease in LV preload due to the inspiratory .
Relatively larger response of ACF RV compared to the LV may be caused by concomitant pulmonary hypertension. No evidence supports RV chamber-specific regulation of protein .
The lung volume effect on PVR takes on special significance when the RV is in a compensated, but precarious, state. In these settings, the added impact of excessive (or .lung expansion lv rv lressureEnhanced systolic LV performance produces greater atrioventricular plane displacement and supports LA reservoir volume expansion, and diastolic LV pressure decay augments the .Breathing-induced changes in intrathoracic pressures influence left ventricular (LV) and right ventricular (RV) volumes, the exact nature and extent of which have not previously .
As the heart and lungs lie in close proximity, increased intrathoracic pressure with mechanical ventilation or forced expiration (e.g., patients with emphysematous lungs) .RV size is measured at end-diastole and the mid-RV diameter is measured at the level of the LV papillary muscles; a diameter of >35 mm is considered abnormal. TTE should provide .
In 1616, Sir William Harvey was the first to describe the importance of right ventricular (RV) function in his seminal treatise, De Motu Cordis: “Thus the right ventricle may be said to be made for the sake of transmitting blood .with RV dilatation, generally presenting normal values in patients with a lower clot burden. Conversely, TAPSE can be decreased even when RV systolic pressure is within the normal range [14], while s′ velocity is generally more specific, with values below the lower limit present only when RV pressure is increased [15]. This finding reflects
Figure 2. Differences between right ventricular (RV) and left ventricular (LV) response to increasing afterload (left panel) and increasing preload (right panel).RV stroke volume falls sharply as mean vascular pressure is increased from 20 to 30 mm Hg in the pulmonary artery, but LV stroke volume stays fairly constant as mean aortic pressure is increased .Introduction. In 1943, after severely damaging the free wall of the right ventricle (RV) with a “red-hot soldering iron,” Starr et al. noted only minimal increases in peripheral venous pressure. This and similar experiments led to the conclusion that “a normal, contractile right ventricular wall is not necessary for the maintenance of a normal circulation” , a concept .
LV and RV share a muscular septum – contributes 20-40% of the work of RV contraction when LV contracts; Dilated failing RV pushes IV septum into LV impairing LV filling/contractility and also impairing role of RV septum on RV contractility; RV Spiral Of Death . RV ischemia is the common final pathway that contributes to progressively . Pulmonary embolism (PE) is a common condition with an incidence exceeding 1 in 1000 and a mortality rate of >15% in the first 3 months after diagnosis. It has a wide clinical spectrum ranging from asymptomatic, small PE to large, life-threatening causing haemodynamic instability and cardiogenic shock. Early diagnosis is therefore .
Pulmonary compliance, a measure of the expansion of the lung, is critical to the proper function of the respiratory system. Lung compliance can be calculated by dividing volume by pressure. Factors affecting lung compliance include elasticity from the elastin in connective tissue and surface tension, which is decreased by surfactant .
lung expansion lv rv lressure Cardiopulmonary physiology: why the heart and lungs are Pulmonary compliance, a measure of the expansion of the lung, is critical to the proper function of the respiratory system. Lung compliance can be calculated by dividing volume by pressure. Factors affecting lung compliance include elasticity from the elastin in connective tissue and surface tension, which is decreased by surfactant .
Cardiopulmonary physiology: why the heart and lungs are 1. Introduction. Pulmonary hypertension (PH) frequently occurs in patients undergoing maintenance hemodialysis (HD) [1, 2].Patients with PH may have right ventricular pressure overload manifested as abnormal motion of the interventricular septum, which can be observed on echocardiography [].The left ventricle becomes D .
Figure 22.3.1 – Boyle’s Law: In a gas, pressure increases as volume decreases. Pulmonary ventilation is dependent on three types of pressure: atmospheric, intra-alveolar, and interpleural. Atmospheric pressure is the amount of force that is exerted by gases in the air surrounding any given surface, such as the body. Because of its thinner wall and higher dependence on coronary perfusion pressure, RV perfusion is more vulnerable to increases in wall tension (increased intramural pressure) and systemic hypotension. 3 Therefore, in case of rapid increases in pulmonary pressures, RV overload occurs (e.g. acute cor pulmonale), and the . Lung expansion therapy is a critical component in both preoperative preparation and postoperative recovery for patients undergoing surgical procedures, particularly those involving the thoracic and abdominal regions. The therapy aims to prevent or reverse atelectasis, a condition characterized by the collapse or incomplete . The diastolic pressures although are nearly equal but with a difference of >5 mm Hg in LV and RV end diastolic pressures. LV myocardial involvement results in pulmonary arterial hypertension > 50 mm Hg unlike CCP. A comparison of hemodynamic abnormalities in CCP and RCMP is summarized in Table 2. In a model of acute pulmonary circulation obstruction mimicking pulmonary embolism, Ghignone et al. (1984) showed that volume expansion was responsible for supplementary rise in RV pressure and decrease in cardiac output. In this study, the perfusion of norepinephrine was able, by restoring arterial pressure, to reduce RV .
INTRODUCTION. Evaluation of the right ventricle (RV) is a key component of the clinical assessment of many cardiovascular and pulmonary disorders. There are many ways to evaluate the RV, most of which can be accomplished noninvasively and without radiation exposure. This topic will discuss the approach to evaluation of RV structure .
Lung expansion therapy is a critical component in both preoperative preparation and postoperative recovery for patients undergoing surgical procedures, particularly those involving the thoracic .
The diastolic pressures although are nearly equal but with a difference of >5 mm Hg in LV and RV end diastolic pressures. LV myocardial involvement results in pulmonary arterial hypertension > 50 mm Hg unlike CCP. A comparison of hemodynamic abnormalities in CCP and RCMP is summarized in Table 2.
In a model of acute pulmonary circulation obstruction mimicking pulmonary embolism, Ghignone et al. (1984) showed that volume expansion was responsible for supplementary rise in RV pressure and decrease in cardiac output. In this study, the perfusion of norepinephrine was able, by restoring arterial pressure, to reduce RV .
INTRODUCTION. Evaluation of the right ventricle (RV) is a key component of the clinical assessment of many cardiovascular and pulmonary disorders. There are many ways to evaluate the RV, most of which can be accomplished noninvasively and without radiation exposure. This topic will discuss the approach to evaluation of RV structure . In 1616, Sir William Harvey was the first physician to realise the importance of the right ventricle (RV) and its interactions with the pulmonary circulation, yet up until the mid-20th century little emphasis had been placed on the RV. Before the 1950s, the main focus was on the left ventricle (LV), the RV being thought of as little more than a . In contrast to the thicker-walled, ellipsoidal-shaped LV, which pumps oxygenated blood at high pressure into the systemic arterial tree, the thinner-walled, crescent-shaped RV pumps deoxygenated blood into a substantially lower pressure, more compliant pulmonary arterial bed. 7,14 The mass of the LV is approximately six times .
Reductions in venous return, right and left ventricular volumes, and LV stroke volume are additional consequences of the altered intra-thoracic pressure gradients [6, 15]. Fig. 3 A schematic diagram showing the potential deleterious effects of lung hyperinflation on cardio-pulmonary interactions in patients with COPD. Equalization of diastolic filling pressures in CP (≤5 mm Hg difference in LV and RV end-diastolic pressure) results from fixed pericardial volume and increased ventricular interdependence (47). However, these criteria have been shown to have poor sensitivity and specificity in differentiating between CP and RCM ( Figure 9 ). At the same time, inspiratory elevation of alveolar pressure and compression of the pulmonary peripheral vessels due to lung inflation have two consequences: 1) an increase in RV afterload (due to an increase in pulmonary system impedance, see Fig. 9 and gray bars in right plot of Fig. 10), and 2) an increase in LV .The right ventricle (RV) because of its low-pressure working conditions and complex geometry stands in stark contrast to the left ventricle (LV). Thus, under normal baseline conditions, the unique anatomy, myocardial ultrastructure, and coronary physiology of the RV reflect a high-volume low-pressure pump.
The ability of the RV to compensate with preserved systolic function in the face of an increasing afterload is referred to as maintaining RV‐PA coupling. 12 Echocardiographic measures of RV‐PA coupling involve the ratio of RV longitudinal motion (ie, TAPSE or TASV)/the RV systolic pressure (RVSP) or PA systolic pressure. 3, 12 . The impact of a dilated RV on LV function becomes critical when the RV is additionally hypertensive. In patients with severe pulmonary arterial hypertension (PAH), RV dilatation compresses the LV within the confines of the relatively fixed, noncompliant, pericardial space, while high RV pressures displace the interventricular septum leftward .
20 Best Watch Blogs and sites. Before we delve into the list, a great app (for .
lung expansion lv rv lressure|Cardiopulmonary physiology: why the heart and lungs are